Fill a Valid Wc 200A Georgia Template
Fill a Valid Wc 200A Georgia Template
Neglecting to file prior forms: Before submitting the WC-200A form, ensure that either Form WC-1 or WC-14 has been filed with the Board. Failing to do so can result in rejection of your request.
Incorrectly filling out identifying information: Double-check the employee's name, claim number, and date of injury. Any discrepancies can delay processing.
Omitting physician details: Make sure to include the names and addresses of both the currently authorized treating physician and the new physician. Missing information can lead to complications.
Not specifying the additional treatment: Clearly state the additional treatment being authorized. Vague descriptions can cause confusion and may result in denial.
Failing to sign the agreement: Ensure that both the employee (or representative) and the employer (or representative) sign the form. Without signatures, the form is not valid.
Ignoring the certificate of service: Remember to certify that copies of the form have been sent to all relevant parties. This step is crucial for compliance.
Not providing accurate contact information: Include correct mailing addresses and email addresses for both the employee and employer. Inaccurate information can hinder communication.
Missing the filing deadline: Submit the form promptly to avoid delays in treatment authorization. Check for any specific timelines that must be adhered to.
What is the purpose of the WC-200A form?
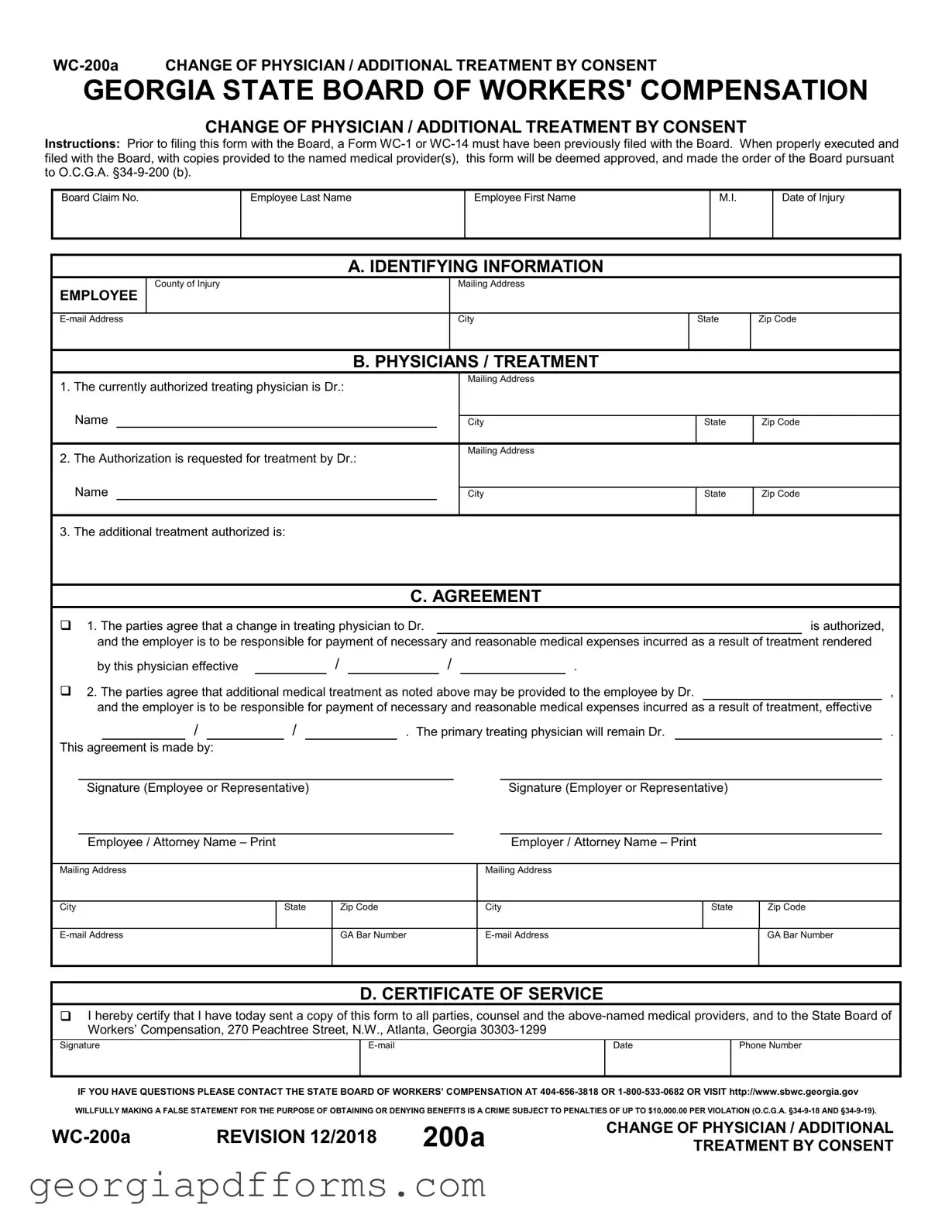
The WC-200A form is used in Georgia to request a change of physician or to authorize additional medical treatment for an employee who is receiving workers' compensation benefits. This form ensures that both the employer and the employee agree on the change or additional treatment, which is crucial for the management of the employee's medical care and related expenses.
When should I file the WC-200A form?
You should file the WC-200A form after you have already submitted a Form WC-1 or WC-14 to the Georgia State Board of Workers' Compensation. This form should be completed and filed before any changes in medical treatment are made. It is essential to ensure that the form is properly executed and filed with the Board to avoid any delays in treatment approval.
Who needs to sign the WC-200A form?
The WC-200A form must be signed by both the employee or their representative and the employer or their representative. This mutual agreement is important as it signifies that both parties consent to the proposed change in physician or the additional treatment. Without these signatures, the form may not be considered valid.
What happens after I submit the WC-200A form?
Once the WC-200A form is properly executed and submitted, it will be deemed approved and made the order of the Board. Copies of the form should be provided to the named medical providers. The employer will then be responsible for payment of necessary and reasonable medical expenses incurred as a result of the treatment rendered by the new physician or for the additional treatment authorized.
Can I change my physician without using the WC-200A form?
No, you cannot change your physician without using the WC-200A form. The form serves as an official request and must be agreed upon by both the employee and employer. Any changes made without this formal consent may lead to complications in your workers' compensation claim and could result in non-payment for medical expenses.
What information is required on the WC-200A form?
The WC-200A form requires several key pieces of information, including the employee's name, date of injury, the currently authorized treating physician's name, and the name of the new physician if applicable. Additionally, the form requires details about the additional treatment authorized and signatures from both parties involved. Accurate and complete information is crucial for the form to be processed smoothly.
What are the consequences of providing false information on the WC-200A form?
Providing false information on the WC-200A form is considered a crime and can lead to severe penalties, including fines of up to $10,000 per violation. It is vital to ensure that all statements made on the form are truthful and accurate to avoid legal repercussions and maintain the integrity of the workers' compensation process.
Workcover Claim - This form is essential for ensuring compliance with Georgia's workers' compensation laws.
Georgia Preliminary Notice of Lien Rights - Filing the notice is a way to protect one's right to payment for services rendered.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
CHANGE OF PHYSICIAN / ADDITIONAL TREATMENT BY CONSENT
Instructions: Prior to filing this form with the Board, a Form
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. IDENTIFYING INFORMATION
EMPLOYEE
County of Injury
Mailing Address
City
State
Zip Code
B. PHYSICIANS / TREATMENT
1.The currently authorized treating physician is Dr.:  Name
Name
2.The Authorization is requested for treatment by Dr.:
Mailing Address
City
Mailing Address
State
Zip Code
Name
City
State
Zip Code
3. The additional treatment authorized is:
C. AGREEMENT
1. The parties agree that a change in treating physician to Dr. |
|
|
|
|
|
|
|
|
is authorized, |
||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment rendered |
||||||||||||||||||||||||
|
by this physician effective |
|
|
|
/ |
|
|
/ |
|
|
. |
|
|
|
|
|
|||||||||
2. The parties agree that additional medical treatment as noted above may be provided to the employee by Dr. |
|
|
, |
||||||||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment, effective |
||||||||||||||||||||||||
|
|
/ |
|
|
|
/ |
|
|
|
|
|
. The primary treating physician will remain Dr. |
|
|
|
. |
|||||||||
This agreement is made by: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Signature (Employee or Representative) |
|
|
|
|
|
|
|
|
|
|
Signature (Employer or Representative) |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Employee / Attorney Name – Print |
|
|
|
|
|
|
|
|
|
|
|
|
Employer / Attorney Name – Print |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
City |
|
State |
|
|
Zip Code |
|
City |
State |
Zip Code |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
GA Bar Number |
|
|
GA Bar Number |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all parties, counsel and the
Signature |
Date |
Phone Number |
|
|
|
|
|
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
200a |
CHANGE OF PHYSICIAN / ADDITIONAL |
|
TREATMENT BY CONSENT |
When completing the WC-200A form in Georgia, consider the following key takeaways:
Be mindful that making false statements on this form can lead to significant penalties.
| Fact Name | Details |
|---|---|
| Form Title | WC-200A Change of Physician / Additional Treatment by Consent |
| Governing Law | O.C.G.A. §34-9-200 (b) |
| Filing Requirement | A Form WC-1 or WC-14 must be filed with the Board prior to submitting this form. |
| Approval Process | When executed properly and submitted, the form is deemed approved by the Board. |
| Medical Provider Notification | Copies of the form must be provided to the named medical provider(s). |
| False Statements Penalty | Willfully making a false statement can lead to penalties of up to $10,000.00 per violation. |