Fill a Valid Georgia Wc 102B Template
Fill a Valid Georgia Wc 102B Template
Omitting Required Information: Failing to fill out all the necessary fields, such as the employee's name, date of injury, or the attorney's contact details, can lead to delays or rejections.
Incorrect Party Identification: Misidentifying the party represented can cause confusion. Ensure that the attorney's name and the party they represent are accurate.
Missing Signature: Forgetting to sign the form is a common mistake. A signature is essential to validate the submission.
Providing Incorrect Contact Information: Double-check that email addresses and phone numbers are correct. Incorrect contact details can hinder communication.
Failing to Notify All Parties: It's crucial to send copies of the completed form to all parties involved. Neglecting this step may lead to legal complications.
Ignoring Submission Deadlines: Be aware of any deadlines for submitting the form. Late submissions can impact the case negatively.
Not Keeping Copies: Always retain a copy of the submitted form for your records. This can be vital if any disputes arise later.
What is the purpose of the Georgia WC-102B form?
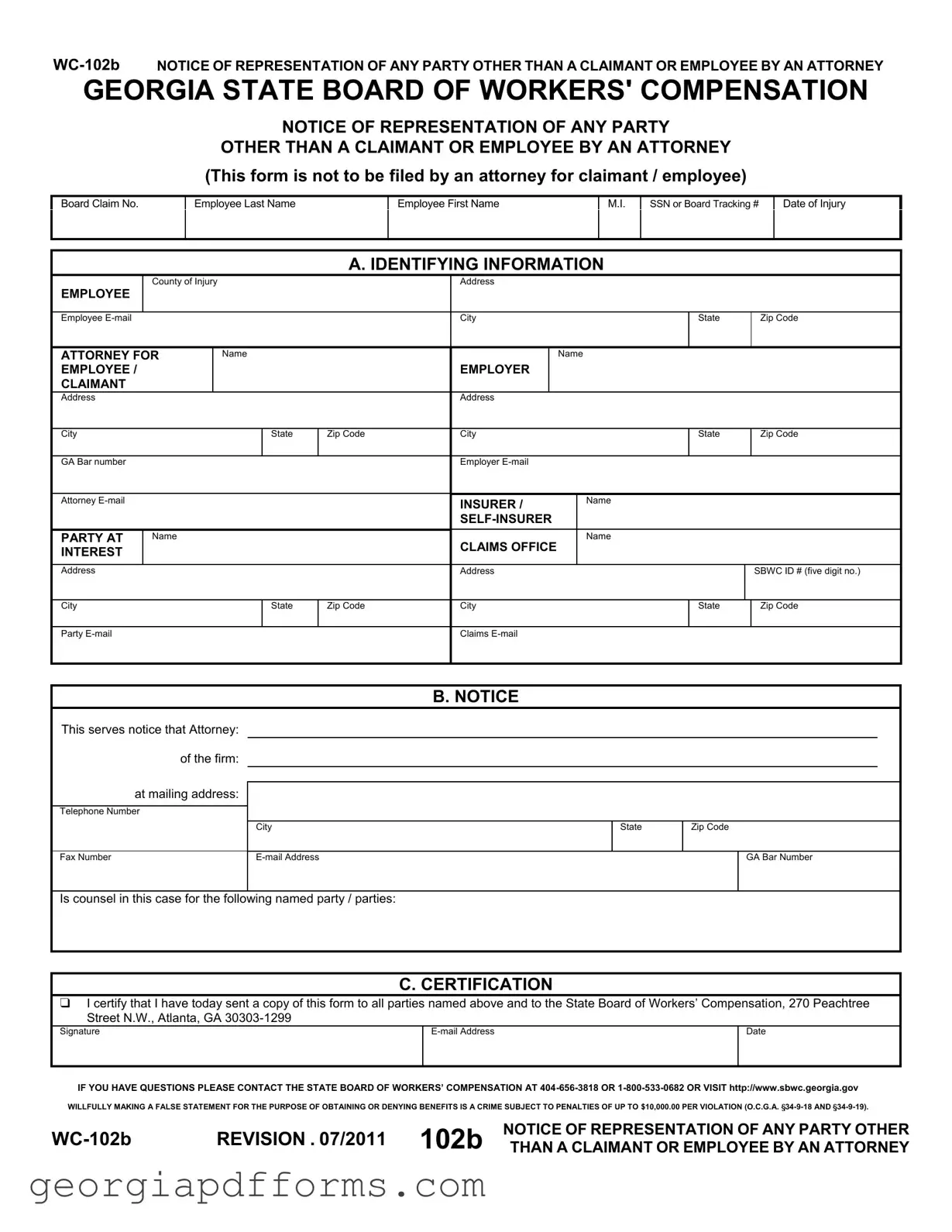
The Georgia WC-102B form serves as a formal notice of representation by an attorney for parties other than the claimant or employee in a workers' compensation case. This form helps to identify the attorney representing a party involved in the case, ensuring that all parties are aware of who is handling the legal aspects of the claim.
Who is required to file the WC-102B form?
This form is specifically not to be filed by an attorney representing the claimant or employee. Instead, it is intended for attorneys representing employers, insurers, or other parties with a vested interest in the case. Filing this form helps clarify the legal representation involved in the workers' compensation process.
What information is needed to complete the WC-102B form?
To complete the WC-102B form, you will need to provide identifying information such as the employee's name, social security number, and details about the injury. Additionally, the attorney’s name, contact information, and the party they represent must be included. This ensures that all relevant parties are documented accurately.
How does one certify the information on the WC-102B form?
Certification on the WC-102B form is done by the attorney completing the form. They must sign it, confirming that they have sent copies of the form to all parties named, as well as to the State Board of Workers’ Compensation. This step is crucial for maintaining transparency and accountability in the process.
What should be done if there are changes in representation?
If there are changes in representation, a new WC-102B form should be filed to reflect the updated information. This ensures that all parties involved in the case are aware of who is representing whom, which is essential for effective communication and legal proceedings.
What are the consequences of providing false information on the WC-102B form?
Providing false information on the WC-102B form is considered a serious offense. It is classified as a crime that can result in penalties of up to $10,000 per violation. This serves as a reminder of the importance of honesty and accuracy when completing legal documents in the workers' compensation process.
Where can I find more information or assistance regarding the WC-102B form?
For additional information or assistance regarding the WC-102B form, you can contact the State Board of Workers’ Compensation at 404-656-3818 or 1-800-533-0682. You may also visit their website at http://www.sbwc.georgia.gov for further resources and guidance.
How to Change Last Name in Georgia After Marriage - Preparedness for the final hearing can impact the court's decision on the name change.
Does Georgia Allow Section 179 Depreciation - Unrelated business income is taxed at a rate of 6% in Georgia.
Georgia Dmv Lien Check - It is advisable for lien holders to keep a copy of the completed form for their records.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
NOTICE OF REPRESENTATION OF ANY PARTY
OTHER THAN A CLAIMANT OR EMPLOYEE BY AN ATTORNEY
(This form is not to be filed by an attorney for claimant / employee)
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
County of Injury
EMPLOYEE
Employee
Address
City
State
Zip Code
ATTORNEY FOR EMPLOYEE / CLAIMANT
Name
EMPLOYER
Name
|
Address |
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip Code |
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar number |
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attorney |
|
|
|
|
INSURER / |
Name |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTY AT |
Name |
|
|
CLAIMS OFFICE |
Name |
|
|||
|
INTEREST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
Address |
|
|
|
SBWC ID # (five digit no.) |
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip Code |
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
Party
Claims
B. NOTICE
This serves notice that Attorney: |
|
|
|
of the firm: |
|
|
|
at mailing address: |
|
|
|
Telephone Number |
|
|
|
|
City |
State |
Zip Code |
Fax Number |
|
GA Bar Number |
Is counsel in this case for the following named party / parties:
C. CERTIFICATION
 I certify that I have today sent a copy of this form to all parties named above and to the State Board of Workers’ Compensation, 270 Peachtree Street N.W., Atlanta, GA
I certify that I have today sent a copy of this form to all parties named above and to the State Board of Workers’ Compensation, 270 Peachtree Street N.W., Atlanta, GA
Signature |
Date |
|
|
|
|
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
REVISION . 07/2011 102b |
NOTICE OF REPRESENTATION OF ANY PARTY OTHER |
|
THAN A CLAIMANT OR EMPLOYEE BY AN ATTORNEY |
Filling out the Georgia WC 102B form is an important step in the workers' compensation process. Understanding how to properly complete and use this form can help ensure that all parties involved are appropriately represented. Here are some key takeaways:
By keeping these takeaways in mind, individuals can navigate the process of using the Georgia WC 102B form more effectively. Proper representation is crucial in workers' compensation cases, and understanding the requirements of this form is a step in the right direction.
| Fact Name | Details |
|---|---|
| Purpose | The WC-102B form is used to notify the Georgia State Board of Workers' Compensation about the representation of a party other than a claimant or employee by an attorney. |
| Governing Law | This form is governed by the Georgia Workers' Compensation Act, specifically O.C.G.A. § 34-9-18 and § 34-9-19. |
| Filing Requirement | Attorneys for parties other than claimants or employees must file this form. Attorneys representing claimants or employees are not required to file it. |
| Information Collected | The form collects identifying information such as the employee's name, date of injury, and details about the attorney and employer. |
| Certification | The attorney must certify that a copy of the form has been sent to all parties involved and to the State Board of Workers' Compensation. |
| Contact Information | For questions regarding the form, individuals can contact the State Board of Workers' Compensation at 404-656-3818 or 1-800-533-0682. |