Fill a Valid Georgia Wc 100 Template
Fill a Valid Georgia Wc 100 Template
Failing to provide complete identifying information. All fields, including names, addresses, and contact details, must be filled out accurately.
Incorrectly entering the Board Claim Number. Ensure that the correct claim number is used to avoid processing delays.
Not indicating whether the claim involves a catastrophic injury designation. This information is crucial for proper handling of the claim.
Omitting the employee's Social Security Number or Board Tracking Number. This information is essential for identification and processing.
Failing to certify participation in mediation. All parties must agree to participate in the mediation process.
Not providing the correct email addresses for all parties involved. Accurate email communication is vital for updates and notifications.
Neglecting to confirm the existence of a valid fee contract. This step is necessary to comply with Board rules.
Forgetting to send a copy of the form to all parties named. This ensures everyone is informed and can prepare for mediation.
Failing to include the signature and date for both the employee representative and the employer/insurer representative. Signatures validate the submission.
Not checking for any updates or changes to the form requirements. Always review the latest guidelines before submission.
What is the Georgia WC-100 form?
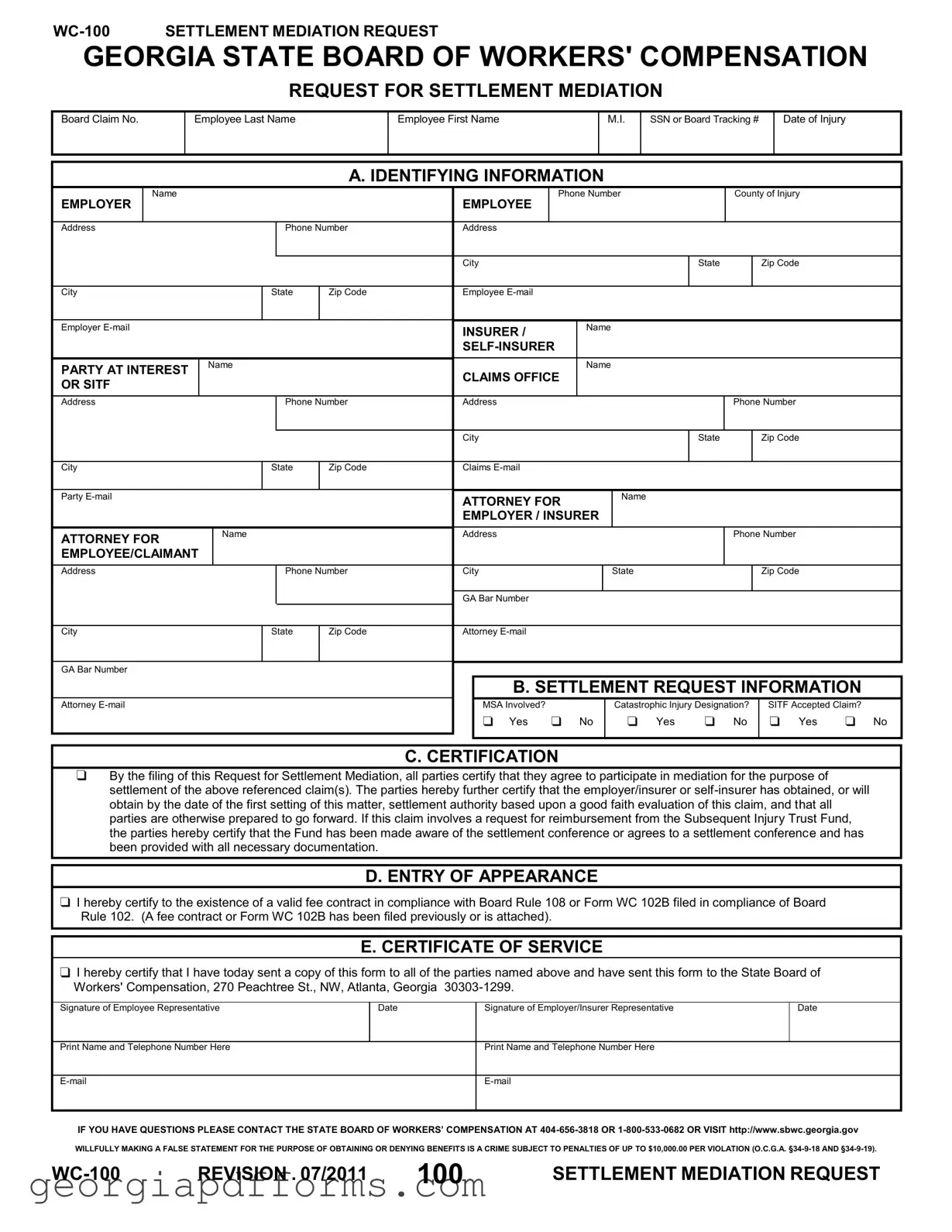
The Georgia WC-100 form is a request for settlement mediation related to workers' compensation claims. It is used by employees and employers to initiate a mediation process aimed at resolving disputes over claims. This form is submitted to the Georgia State Board of Workers' Compensation to facilitate discussions between the involved parties.
Who needs to fill out the WC-100 form?
What information is required on the WC-100 form?
What is the purpose of the mediation request?
How does one certify participation in mediation?
What happens after the form is submitted?
Are there penalties for false statements on the WC-100 form?
Where can I get more information about the WC-100 form?
T-200 - The form can be obtained through the Professional Licensing Boards and Securities Division's website.
How to Change Last Name in Georgia After Marriage - The name change process entails a series of clearly defined steps that must be followed diligently.
Georgia Medicaid Application - The form accommodates various categories, including Pregnant Women and Families with Children.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
REQUEST FOR SETTLEMENT MEDIATION
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
|
|
Name |
|
|
|
|
|
|
Phone Number |
|
County of Injury |
|||
|
EMPLOYER |
|
|
|
|
|
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
Phone Number |
Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Employee |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
|
|
|
INSURER / |
|
Name |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTY AT INTEREST |
Name |
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
CLAIMS OFFICE |
|
|
|
|
|
||||
|
OR SITF |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address |
|
|
Phone Number |
Address |
|
|
|
Phone Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
State |
Zip Code |
Claims |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Party
ATTORNEY FOR |
Name |
|
|
EMPLOYEE/CLAIMANT |
|
|
|
ATTORNEY FOR |
Name |
|
|
EMPLOYER / INSURER |
|
|
|
Address |
|
|
|
Phone Number
Address |
|
Phone Number |
City |
|
State |
|
|
Zip Code |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
Attorney |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. SETTLEMENT REQUEST INFORMATION |
|
|||||
Attorney |
|
|
|
|
MSA Involved? |
|
Catastrophic Injury Designation? |
|
SITF Accepted Claim? |
|
|
|
|
|
|
|
Yes |
No |
Yes |
No |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. CERTIFICATION
By the filing of this Request for Settlement Mediation, all parties certify that they agree to participate in mediation for the purpose of settlement of the above referenced claim(s). The parties hereby further certify that the employer/insurer or
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or Form WC 102B filed in compliance of Board Rule 102. (A fee contract or Form WC 102B has been filed previously or is attached).
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties named above and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Signature of Employee Representative
Date
Signature of Employer/Insurer Representative
Date
Print Name and Telephone Number Here
Print Name and Telephone Number Here
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
100 |
SETTLEMENT MEDIATION REQUEST |
When filling out and using the Georgia WC 100 form, keep these key takeaways in mind:
| Fact Name | Details |
|---|---|
| Form Purpose | The WC-100 form is used to request mediation for settlement in workers' compensation claims in Georgia. |
| Governing Law | This form is governed by the Georgia Workers' Compensation Act (O.C.G.A. §34-9). |
| Claim Information | It requires specific claim information, including the Board Claim Number and details about the employee and employer. |
| Involved Parties | All parties involved must provide their contact information, including names, addresses, and emails. |
| Settlement Authority | Employers or insurers must certify that they have obtained settlement authority before mediation. |
| Certification Requirement | Filing the form certifies that all parties agree to participate in mediation. |
| Subsequent Injury Trust Fund | If applicable, the form must indicate whether the Subsequent Injury Trust Fund has been notified of the mediation. |
| Fee Contract | A valid fee contract must exist, in compliance with Board Rule 108 or Form WC 102B. |
| False Statements Penalty | Providing false information can lead to penalties of up to $10,000 per violation (O.C.G.A. §34-9-18 and §34-9-19). |