Fill a Valid Georgia Dma 6 Template
Fill a Valid Georgia Dma 6 Template
Failing to provide complete identifying information. All sections, including the applicant's name, address, Medicaid number, and Social Security number, must be filled out accurately.
Not including the correct birthdate. It is essential to enter the applicant's birthdate to avoid delays in processing.
Omitting the primary care physician's information. This information is critical for coordinating care and verifying medical history.
Inaccurately answering questions regarding the applicant's school attendance and institutionalization. These answers must reflect the current situation to ensure appropriate care recommendations.
Not signing or dating the authorization section. The signature of the parent or legal representative is necessary for the form to be valid.
Failing to attach required documentation, such as medical records or additional sheets for history and diagnosis. This can lead to incomplete evaluations.
Leaving out details about medications and treatment plans. Accurate medication information is crucial for assessing the applicant's needs.
Not checking the appropriate boxes in the evaluation of nursing care needed section. This oversight can misrepresent the level of care required.
Providing incomplete or inaccurate physician information, including licensure number and contact details. This information is necessary for follow-up and verification purposes.
What is the Georgia DMA 6 form?
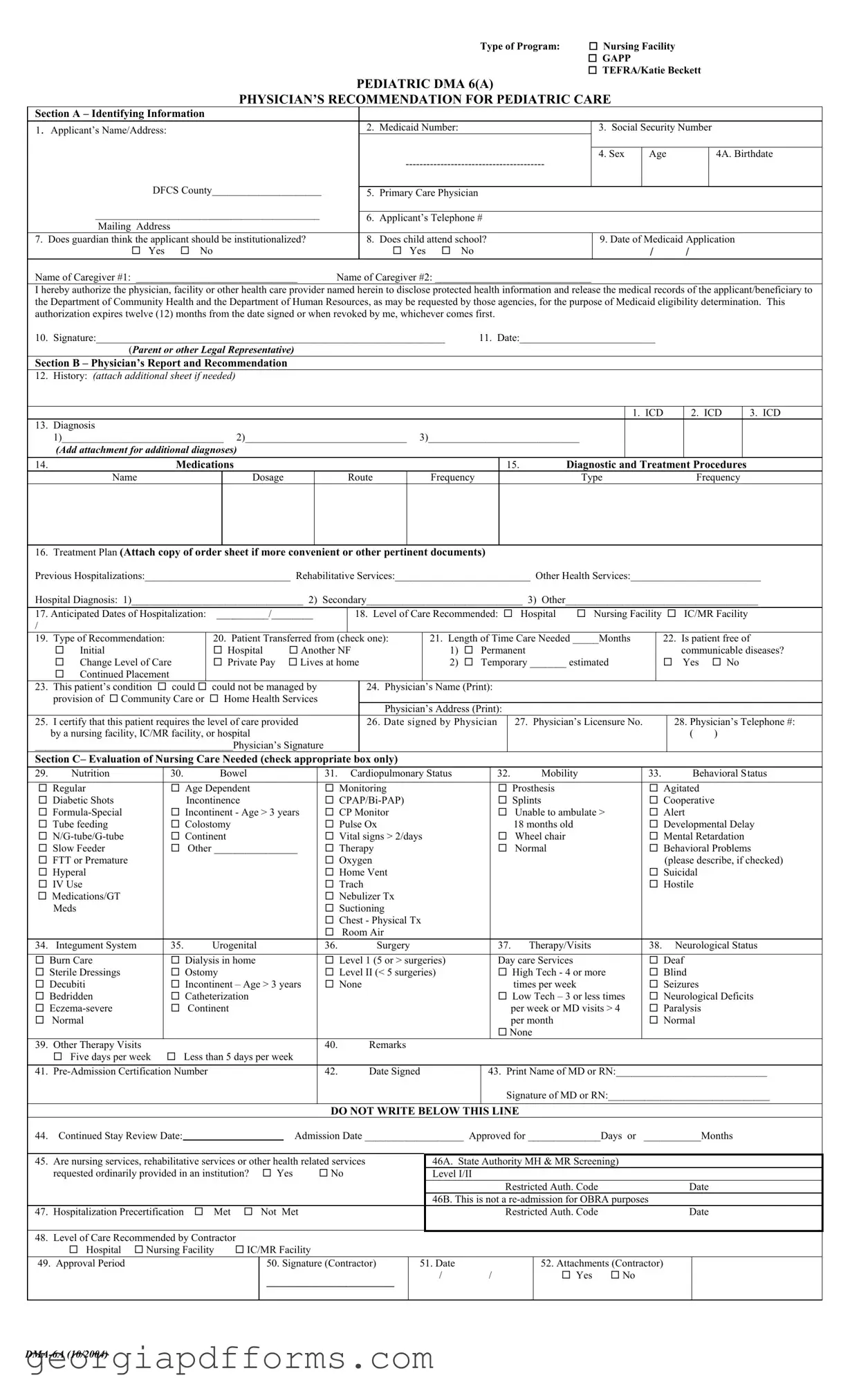
The Georgia DMA 6 form is a document used for the Medicaid eligibility determination process for children who require nursing facility care. It collects essential information about the applicant, including medical history, diagnosis, and the level of care needed.
Who needs to fill out the DMA 6 form?
This form must be completed by a physician who is familiar with the applicant's medical condition. It is intended for children who may need institutional care or specialized services under Medicaid programs such as GAPP, TEFRA, or Katie Beckett.
What information is required in Section A of the DMA 6 form?
Section A requires identifying information about the applicant, including their name, address, Medicaid number, Social Security number, age, and birthdate. It also asks for the primary care physician's details and whether the guardian believes the applicant should be institutionalized.
What should be included in Section B of the DMA 6 form?
Section B focuses on the physician's report and recommendation. It includes the applicant's medical history, diagnoses, medications, treatment plans, and anticipated dates of hospitalization. Physicians should also indicate the recommended level of care and whether the applicant's condition can be managed with community care or home health services.
How does the DMA 6 form support Medicaid eligibility determination?
The DMA 6 form provides the necessary medical documentation to support a child's application for Medicaid services. The information collected helps the Department of Community Health and the Department of Human Resources assess the applicant's medical needs and eligibility for coverage.
What happens if the form is incomplete or inaccurate?
If the DMA 6 form is incomplete or contains inaccuracies, it may delay the eligibility determination process. It is crucial to ensure that all sections are filled out accurately and completely to avoid any complications.
How long is the authorization for disclosure of medical records valid?
The authorization for the disclosure of protected health information is valid for twelve months from the date it is signed or until it is revoked by the legal representative, whichever comes first.
What is the significance of the physician's signature on the DMA 6 form?
The physician's signature on the DMA 6 form certifies that the information provided is accurate and that the applicant requires the level of care specified. This endorsement is essential for the Medicaid application process.
Can additional information be attached to the DMA 6 form?
Yes, additional sheets can be attached to provide more detailed medical history, diagnoses, or treatment plans. This information can help clarify the applicant's needs and support the eligibility determination.
What should be done after completing the DMA 6 form?
Once the DMA 6 form is completed, it should be submitted to the appropriate Medicaid agency along with any other required documentation. It is advisable to keep a copy for personal records.
Mv-6 - Understanding the requirements will facilitate a smoother application process.
In the realm of transactions, having a clear understanding of the process is essential, and utilizing resources like OnlineLawDocs.com can greatly assist in acquiring a proper Georgia Bill of Sale form to facilitate the ownership transfer smoothly.
How to Change Last Name in Georgia After Marriage - Understand the distinctions between Legitimation and Name Change processes to avoid confusion.
Georgia Workers' Compensation Forms - This form reaffirms the rights and responsibilities of injured employees under Georgia's work compensation system.
|
|
|
|
|
|
Type of Program: |
Nursing Facility |
|
|
|
|
|
|
|
|
|
|
GAPP |
|
|
|
|
|
|
|
|
|
|
TEFRA/Katie Beckett |
|||
|
|
|
PEDIATRIC DMA 6(A) |
|
|
|
|
|||
|
|
PHYSICIAN’S RECOMMENDATION FOR PEDIATRIC CARE |
|
|
|
|||||
Section A – Identifying Information |
|
|
|
|
|
|
|
|
||
1. |
Applicant’s Name/Address: |
|
|
2. |
Medicaid Number: |
|
3. Social Security Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Sex |
Age |
|
4A. Birthdate |
|
|
|
|
|
|
|
|
|
||
|
DFCS County_____________________ |
|
|
|
|
|
|
|
|
|
|
|
5. |
Primary Care Physician |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
___________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
6. |
Applicant’s Telephone # |
|
|
|
|
|||
|
Mailing Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
7. |
Does guardian think the applicant should be institutionalized? |
|
8. |
Does child attend school? |
9. Date of Medicaid Application |
|||||
|
Yes |
No |
|
|
Yes |
No |
|
/ |
/ |
|
Name of Caregiver #1: _______________________________ |
Name of Caregiver #2: ______________________________ |
|
|
|
|
|||||
I hereby authorize the physician, facility or other health care provider named herein to disclose protected health information and release the medical records of the applicant/beneficiary to the Department of Community Health and the Department of Human Resources, as may be requested by those agencies, for the purpose of Medicaid eligibility determination. This authorization expires twelve (12) months from the date signed or when revoked by me, whichever comes first.
10. Signature:___________________________________________________________________ |
11. Date:__________________________ |
(Parent or other Legal Representative) |
|
Section B – Physician’s Report and Recommendation
12. |
History: (ATTACH ADDITIONAL SHEET IF NEEDED) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. ICD |
|
|
2. ICD |
|
3. ICD |
||||
13. |
Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1)_______________________________ 2)_______________________________ 3)_____________________________ |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
(Add attachment for additional diagnoses) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
14. |
|
|
|
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
|
Diagnostic and Treatment Procedures |
||||||||||||||||||
|
|
Name |
|
|
|
|
|
|
|
Dosage |
|
|
|
Route |
|
|
Frequency |
|
|
|
|
|
|
Type |
|
|
|
Frequency |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
16. |
Treatment Plan (Attach copy of order sheet if more convenient or other pertinent documents) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
Previous Hospitalizations:____________________________ Rehabilitative Services:__________________________ Other Health Services:_________________________ |
||||||||||||||||||||||||||||||||||||||||
|
Hospital Diagnosis: 1)_________________________________ 2) Secondary______________________________ 3) Other_____________________________________ |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
17. Anticipated Dates of Hospitalization: |
__________/________ |
|
|
|
18. |
Level of Care Recommended: |
Hospital |
Nursing Facility |
|
|
IC/MR Facility |
|||||||||||||||||||||||||||||
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. |
Type of Recommendation: |
|
|
|
20. Patient Transferred from (check one): |
|
21. Length of Time Care Needed _____Months |
|
22. Is patient free of |
||||||||||||||||||||||||||||||||
|
|
Initial |
|
|
|
|
|
|
|
Hospital |
|
Another NF |
|
|
|
1) |
Permanent |
|
|
|
|
|
|
|
communicable diseases? |
||||||||||||||||
|
|
Change Level of Care |
|
|
|
Private Pay |
|
Lives at home |
|
|
|
2) |
Temporary _______ estimated |
|
|
Yes |
|
No |
|||||||||||||||||||||||
|
|
Continued Placement |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
23. |
This patient’s condition |
could |
could not be managed by |
|
|
24. Physician’s Name (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
provision of |
Community Care or |
|
Home Health Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Address (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
25. |
I certify that this patient requires the level of care provided |
|
|
26. Date signed by Physician |
|
27. |
|
Physician’s Licensure No. |
|
28. Physician’s Telephone #: |
|||||||||||||||||||||||||||||||
|
by a nursing facility, IC/MR facility, or hospital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|||||||||||||
|
______________________________________Physician’s Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Section C– Evaluation of Nursing Care Needed (check appropriate box only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29. |
Nutrition |
|
|
|
30. |
|
|
Bowel |
|
|
|
|
|
|
31. Cardiopulmonary Status |
|
32. |
|
|
Mobility |
|
33. |
|
|
|
Behavioral Status |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Regular |
|
|
|
|
Age Dependent |
|
|
|
|
Monitoring |
|
|
|
|
|
|
Prosthesis |
|
|
|
|
Agitated |
|
|
|
||||||||||||||
|
|
Diabetic Shots |
|
|
|
|
Incontinence |
|
|
|
|
|
|
|
|
|
|
|
|
Splints |
|
|
|
|
Cooperative |
|
|
||||||||||||||
|
|
|
|
|
Incontinent - Age > 3 years |
|
CP Monitor |
|
|
|
|
|
|
Unable to ambulate > |
|
Alert |
|
|
|
||||||||||||||||||||||
|
|
Tube feeding |
|
|
|
|
Colostomy |
|
|
|
|
|
|
Pulse Ox |
|
|
|
|
|
|
18 months old |
|
|
|
|
Developmental Delay |
|||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
Vital signs > 2/days |
|
|
|
|
Wheel chair |
|
|
|
|
Mental Retardation |
|||||||||||||||||||
|
|
Slow Feeder |
|
|
|
|
Other ________________ |
|
Therapy |
|
|
|
|
|
|
Normal |
|
|
|
|
Behavioral Problems |
||||||||||||||||||||
|
|
FTT or Premature |
|
|
|
|
|
|
|
|
|
|
|
|
|
Oxygen |
|
|
|
|
|
|
|
|
|
|
|
|
|
(please describe, if checked) |
|||||||||||
|
|
Hyperal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Vent |
|
|
|
|
|
|
|
|
|
|
|
|
|
Suicidal |
|
|
|
|||||||
|
|
IV Use |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trach |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hostile |
|
|
|
|||||
|
|
Medications/GT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nebulizer Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Meds |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest - Physical Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room Air |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
34. |
Integument System |
|
|
35. |
|
|
Urogenital |
|
|
|
|
36. |
|
|
Surgery |
|
|
|
37. |
|
Therapy/Visits |
|
38. |
|
Neurological Status |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Burn Care |
|
|
|
|
Dialysis in home |
|
|
|
|
Level 1 (5 or > surgeries) |
|
Day care Services |
|
|
|
|
Deaf |
|
|
|
||||||||||||||||||||
|
Sterile Dressings |
|
|
|
|
Ostomy |
|
|
|
|
|
|
Level II (< 5 surgeries) |
|
|
|
|
High Tech - 4 or more |
|
Blind |
|
|
|
||||||||||||||||||
|
Decubiti |
|
|
|
|
Incontinent – Age > 3 years |
|
None |
|
|
|
|
|
|
|
|
times per week |
|
|
|
|
Seizures |
|
|
|
||||||||||||||||
|
Bedridden |
|
|
|
|
Catheterization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low Tech – 3 or less times |
|
Neurological Deficits |
|||||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per week or MD visits > 4 |
|
Paralysis |
|
|
|
||||||||||||||
|
|
Normal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per month |
|
|
|
|
Normal |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
|
|||
39. |
Other Therapy Visits |
|
|
|
|
|
|
|
|
|
|
|
|
|
40. |
|
|
Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Five days per week |
|
Less than 5 days per week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
41. |
|
|
|
|
|
|
|
|
42. |
|
|
Date Signed |
43. Print Name of MD or RN:_____________________________ |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of MD or RN:_______________________________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE BELOW THIS LINE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
44. |
Continued Stay Review Date: |
|
|
|
|
|
|
|
Admission Date ___________________ Approved for ______________Days or ___________Months |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. |
Are nursing services, rehabilitative services or other health related services |
|
|
|
46A. State Authority MH & MR Screening) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
requested ordinarily provided in an institution? |
Yes |
No |
|
|
|
Level I/II |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
46B. This is not a |
|
|
|
|
|
|
|
|||||||||||
47. |
Hospitalization Precertification |
|
|
Met |
|
Not |
Met |
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
48. |
Level of Care Recommended by Contractor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Hospital |
Nursing Facility |
IC/MR Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
49. |
Approval Period |
|
|
|
|
|
|
|
|
50. Signature (Contractor) |
|
51. Date |
|
|
|
|
|
|
52. Attachments (Contractor) |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
________________ |
|
/ |
/ |
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Filling out the Georgia DMA 6 form is an important step for families seeking Medicaid assistance for pediatric care. Here are some key takeaways to keep in mind:
Completing the Georgia DMA 6 form accurately and thoroughly can significantly impact the outcome of the Medicaid application. Take your time to ensure that all information is correct and complete.
| Fact Name | Description |
|---|---|
| Form Purpose | The Georgia DMA 6 form is used to recommend pediatric care for applicants needing nursing facility services under Medicaid. |
| Governing Law | This form operates under Georgia Medicaid regulations, specifically the Georgia Department of Community Health guidelines. |
| Applicant Information | Section A requires identifying information such as the applicant's name, address, Medicaid number, and social security number. |
| Physician's Role | A physician must complete the form, providing a recommendation and medical history to support the applicant's need for care. |
| Authorization | The form includes an authorization section allowing the disclosure of protected health information to relevant health agencies. |
| Caregiver Information | It requires the names and contact information of caregivers involved in the applicant's care. |
| Diagnosis Documentation | Physicians must document the applicant's diagnoses using ICD codes, which are critical for Medicaid eligibility. |
| Evaluation of Care Needs | Section C evaluates the nursing care needed, including nutrition, mobility, and behavioral status among other factors. |