Fill a Valid Georgia Application For Medicaid Template
Fill a Valid Georgia Application For Medicaid Template
Incomplete Personal Information: Failing to fill out all sections of personal information can lead to delays. Ensure that every field, including names, addresses, and contact information, is completed accurately.
Missing Signatures: Not signing the application is a common oversight. Remember, both the applicant and their spouse (if applicable) must sign the form.
Incorrect or Missing Social Security Numbers: Providing incorrect Social Security numbers can cause significant issues. Double-check that all numbers are accurate and complete.
Omitting Assets and Resources: Failing to disclose all assets, such as real estate or vehicles, can lead to disqualification. Be thorough when listing resources owned by you or your spouse.
Neglecting to Report Income: Underreporting or omitting income sources may result in complications. List all income sources and amounts before deductions.
Forgetting to Attach Necessary Documentation: Not including required documents, such as Medicare cards or proof of income, can stall the application process. Gather and attach all necessary paperwork.
Not Providing Accurate Contact Information: If the contact number is incorrect, the Medicaid Specialist may have trouble reaching you for follow-up questions or interviews.
Ignoring the Privacy Statement: Failing to understand the privacy statement can lead to confusion about how personal information will be used. Take time to read and comprehend these terms.
What is the Georgia Application for Medicaid form?
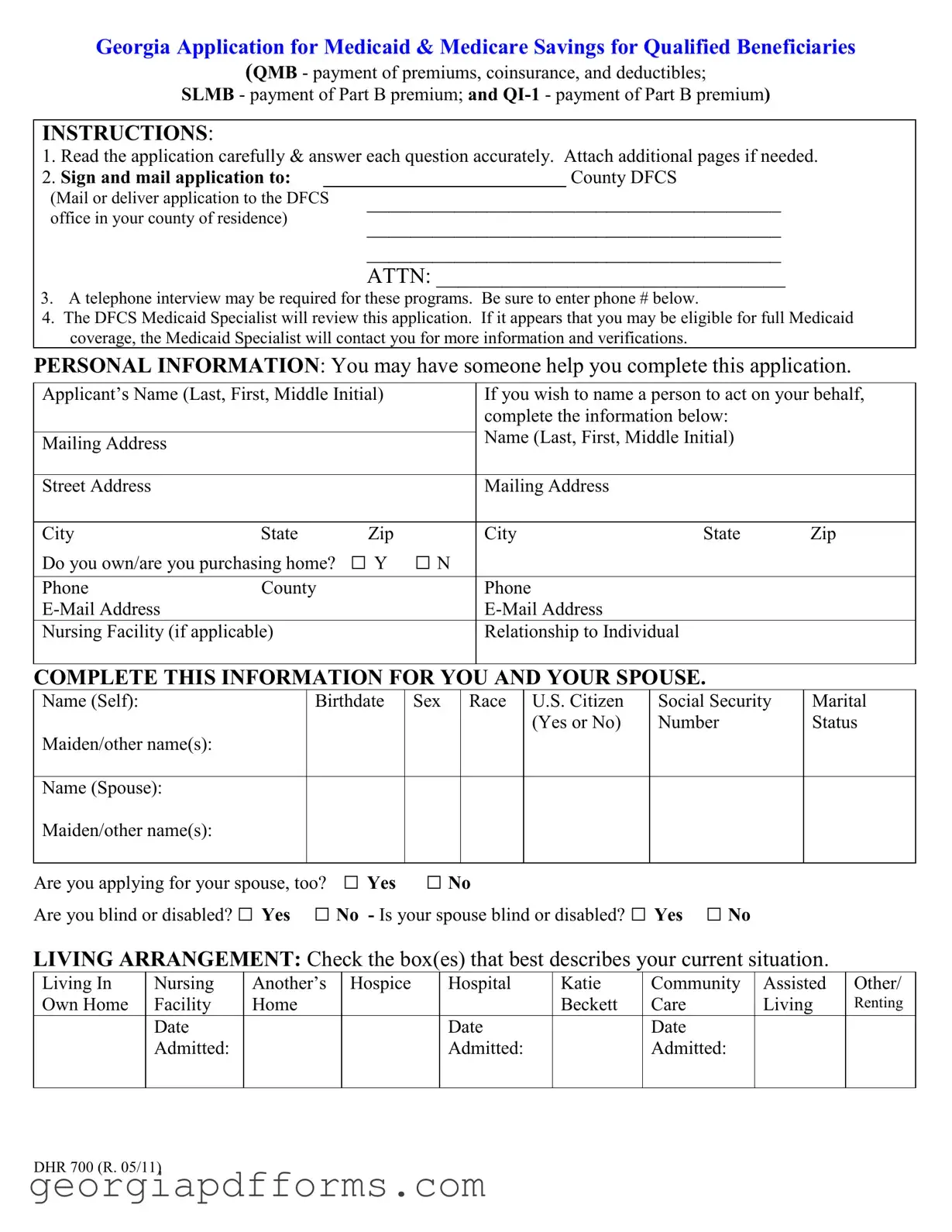
The Georgia Application for Medicaid form is used to apply for Medicaid and Medicare Savings programs for qualified beneficiaries. This includes assistance with premiums, coinsurance, and deductibles for Medicare. It is essential for individuals seeking financial support for healthcare services.
Who can help me complete the application?
You may have someone assist you in completing the application. This could be a family member, friend, or caregiver. Ensure that the person helping you is aware of your personal information and can accurately provide the necessary details.
Where should I send my completed application?
After filling out the application, sign it and mail it to your local County Department of Family and Children Services (DFCS) office. You can also deliver it in person. Make sure to check the address for your specific county.
Will I need to participate in a telephone interview?
A telephone interview may be required as part of the application process. If so, be prepared to provide additional information. It is important to include your phone number on the application so the Medicaid Specialist can reach you if needed.
What happens after I submit my application?
The DFCS Medicaid Specialist will review your application. If it seems you may qualify for full Medicaid coverage, they will contact you for further information and verification. This may include documentation of income, resources, and living arrangements.
What information do I need to provide about my income?
You must list all types of income you and your spouse receive before any deductions. This includes Social Security, wages, pensions, and any other benefits. Be sure to provide the amount and frequency of each income source.
What if I have other health insurance?
If you or your spouse have other health insurance, you must indicate this on the application. You will need to provide details about the insurance type, coverage, and effective dates. Attach copies of your insurance cards if applicable.
What are the privacy protections for my information?
Your information is protected by federal and state laws. These laws limit the use and disclosure of your confidential information to purposes directly related to the administration of Medicaid programs. Only authorized personnel will access your information for eligibility determination.
What if I need to make changes after submitting my application?
If your income, resources, or living arrangements change after submitting your application, you are required to notify the agency. This ensures that your eligibility is accurately assessed and maintained.
Where to Send Form 4506-t - Filing the 4506 form correctly ensures timely processing of your request.
Georgia T 129 - Ultimately, the T 129 form reinforces safety standards for drivers and vehicle owners across Georgia.
Georgia Application for Medicaid & Medicare Savings for Qualified Beneficiaries
(QMB - payment of premiums, coinsurance, and deductibles;
SLMB - payment of Part B premium; and
INSTRUCTIONS:
1. Read the application carefully & answer each question accurately. Attach additional pages if needed.
2. Sign and mail application to: __________________________ County DFCS
(Mail or deliver application to the DFCS office in your county of residence)
______________________________________
______________________________________
______________________________________
ATTN: ________________________________
3.A telephone interview may be required for these programs. Be sure to enter phone # below.
4.The DFCS Medicaid Specialist will review this application. If it appears that you may be eligible for full Medicaid coverage, the Medicaid Specialist will contact you for more information and verifications.
PERSONAL INFORMATION: You may have someone help you complete this application.
Applicant’s Name (Last, First, Middle Initial) |
|
If you wish to name a person to act on your behalf, |
||||
|
|
|
|
complete the information below: |
|
|
|
|
|
|
Name (Last, First, Middle Initial) |
|
|
Mailing Address |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
City |
State |
Zip |
|
City |
State |
Zip |
Do you own/are you purchasing home? |
□ Y |
□ N |
|
|
|
|
Phone |
County |
|
|
Phone |
|
|
|
|
|
|
|
||
Nursing Facility (if applicable) |
|
|
Relationship to Individual |
|
|
|
|
|
|
|
|
|
|
COMPLETE THIS INFORMATION FOR YOU AND YOUR SPOUSE.
Name (Self): |
Birthdate |
Sex |
Race |
U.S. Citizen |
Social Security |
Marital |
|
|
|
|
(Yes or No) |
Number |
Status |
Maiden/other name(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name (Spouse): |
|
|
|
|
|
|
Maiden/other name(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
Are you applying for your spouse, too? □ Yes |
□ No |
|
|
|||
Are you blind or disabled? □ Yes |
□ No - Is your spouse blind or disabled? □ Yes □ No |
|
||||
LIVING ARRANGEMENT: Check the box(es) that best describes your current situation.
Living In |
Nursing |
Another’s |
Hospice |
Hospital |
Katie |
Community |
Assisted |
Other/ |
Own Home |
Facility |
Home |
|
|
Beckett |
Care |
Living |
Renting |
|
Date |
|
|
Date |
|
Date |
|
|
|
Admitted: |
|
|
Admitted: |
|
Admitted: |
|
|
|
|
|
|
|
|
|
|
|
DHR 700 (R. 05/11)
HEALTH INSURANCE:
Do you have Medicare? |
Type of Coverage |
Effective Date: |
Have you ever |
|||
□ Yes |
□ No |
□ Part A |
□ Part B |
______________ |
received SSI? |
|
Are you enrolled in a Medicare |
(hospital) |
(doctor) |
|
□ Yes |
□ No |
|
HMO or Medicare Drug program? |
Part D |
|
Medicare Number: |
If so, when did it |
||
□ Yes |
□ No |
(RX) |
|
____________ |
end?________ |
|
|
|
|
|
|
|
|
|
|
|
|
|||
Does your spouse have |
Type of Coverage |
Effective Date: |
Has your spouse |
|||
Medicare? |
□ No |
□ Part A |
□ Part B |
______________ |
ever received SSI? |
|
□ Yes |
Part D |
|
Medicare Number: |
□ Yes |
□ No |
|
|
|
|
If so, when did it |
|||
|
|
|
|
____________ |
end?________ |
|
|
|
|
|
|
|
|
Do you have other health insurance? |
□ Yes |
□ No |
Does your spouse have other health insurance? |
□ Yes |
□ No |
If you answered yes to either of these questions, please complete the following information:
|
Health Insurance |
Type of Coverage |
Effective |
Policy |
|
Company Name, |
(Hospital, Medicare |
Date |
Number |
|
Address, and Telephone |
Supplement, Drugs, Major |
|
|
|
Number |
Medical,) |
|
|
Self |
|
|
|
|
|
|
|
|
|
Spouse |
|
|
|
|
|
|
|
|
|
Attach copies (front and back) of Medicare and insurance cards if applicable.
REAL PROPERTY: Do you own all or part of any real estate in which you do not live?□ Yes □ No If yes, please complete the following for each piece of real estate. Do not list the house or mobile home in which you live.
Address |
Value |
Amount Owed |
|
|
|
|
|
|
Do you or your spouse own a car, truck, boat, camper, utility trailer, recreational vehicle, etc.?
□ Yes |
□ No If yes, please complete the following information about each vehicle. Attach |
|||||
additional pages if needed. |
|
|
|
|||
Type |
|
Year |
Make |
Model |
Value |
Amount Owed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DHR 700 (R. 05/11)
RESOURCES: Check all resources (assets) owned by you, your spouse, or jointly owned with someone else. Include any accounts or properties on which your name(s) appear. Attach additional pages if necessary.
Do you or your spouse have any of the following resources?
Checking account |
□ Yes |
□ No |
Funeral plans/ prepaid burial item |
□ Yes |
□ No |
Savings account |
□ Yes |
□ No |
Burial plots or contracts |
□ Yes |
□ No |
Government bonds |
□ Yes |
□ No |
Stocks and bonds |
□ Yes |
□ No |
Trust funds |
□ Yes |
□ No |
Other (IRA, CD, promissory note, etc.) |
□ Yes |
□ No |
Have you or your spouse given away any assets for less than its value? |
□ Yes |
□ No |
|||
If you answered yes to any of these questions, describe below. Attach additional pages if necessary.
Type of Resource |
|
Account/ Policy |
Value |
Name of Bank, Insurance Company, |
||||
|
|
Number |
|
Etc. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you or your spouse have a life insurance policy? |
|
□ Yes |
□ No |
|||||
If yes, please complete the following information. Attach additional pages if necessary. |
|
|||||||
Policy Owner |
Insurance Company |
|
Policy Number |
Face |
|
Cash Value |
||
|
|
|
|
|
|
Value |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INCOME AND EARNINGS: List all types of earnings and income that you and your spouse receives. List the income amount before deductions (such as taxes, insurance, or Medicare premiums) are taken out. Attach additional pages if needed. Income includes, but is not limited to:
Social Security |
|
SSI |
Wages/ |
|
Railroad Retirement Benefits |
Veterans’ Benefits |
Trust or Annuity Payments |
||
Pensions/ Retirement Benefits |
Rental Income Paid to You |
Oil Royalties/ Mineral Rights |
||
Name of |
Type of |
Source of Income or Amount |
How Often |
Claim Number |
Person Who |
Income |
Name of Employer |
Received? |
(if applicable) |
Receives |
|
|
(weekly, |
|
Income |
|
|
monthly, etc.) |
|
|
|
|
|
|
Are you a veteran? □ Yes □ No Is your spouse a veteran? Yes No
Where did you and spouse work in the past? ____________________________________________________
Do you or your spouse have any unpaid medical bills ? |
□ Yes □ No |
DHR 700 (R. 05/11)
PRIVACY STATEMENT:
Federal and state laws and regulations limit the use and disclosure of confidential information concerning applicants and recipients of all agency programs to purposes directly related to the administration of these programs.
ASSIGNMENT OF RIGHTS OF PAYMENT FOR MEDICAL SUPPORT AND OTHER MEDICAL CARE:
(If you are applying on behalf of another individual and do not have the power to execute an assignment for that individual, the individual will need to execute an assignment of the rights described below, as a condition of his or her eligibility for the benefits covered by this application.) As a condition of my eligibility, I agree to assign to the
State all rights to medical support and to payment for medical care from any third party (hospital and medical benefits). I agree to cooperate with the state in identifying and providing information to assist the state in pursuing any third party who may be liable to pay for care and services. I understand that I must report any payments received for medical care within ten days.
APPLICANT’S STATEMENT OF UNDERSTANDING AND AGREEMENT:
I understand that, by signing this application, I am agreeing to a full investigation or review of my eligibility by state and/or federal officials. This may include inquiries of employers, medical providers, financial institutions, and other business and professional persons and review of any agency records. I also agree that my application authorizes these agencies to release to this agency the information needed to determine my eligibility. I agree to provide the documents necessary to establish eligibility. If documents are not available, I agree to give the name of the person or organization from which this agency may obtain the necessary proof.
I understand that each individual who receives assistance must provide or apply for a Social Security Number. I authorize the use of my (our) Social Security Number for such purposes as identification, program reviews or audits, and computer matching with other agencies and institutions such as banks, saving and loan associations, and other government agencies, including Internal Revenue Service, to verify eligibility for assistance.
I understand that my application will be considered without regard to race, color, sex, age, handicap, religion, national origin, or political belief. I understand that I may request a fair hearing if I disagree with an agency decision in my case and that I may be represented by any person I choose.
I understand that Medicaid members who, are an inpatient in a nursing facility, intermediate care facility for
the mentally retarded, or other mental institution that have their medical care paid by Medicaid will be subject to the Medicaid Estate Recovery Program. Additionally, Medicaid members who are 55 years of age or older and who receive home and community based services or are enrolled in and receive services through a waiver program are also subject to Estate Recovery. I acknowledge receipt of a written notice that medical assistance payments made on my behalf may be recovered from my estate after my death.
I certify that I (or if filing for my spouse, my spouse and I) am a U.S. citizen, national, or alien in qualified alien status. If this application is being filed on behalf of another individual or individuals, the actual applicant(s) will need to make this certification.
APPLICANT(S) OR REPRESENTATIVE MUST READ AND SIGN:
State and federal law provide for fine, imprisonment, or both for any person who withholds or gives false information to obtain assistance to which he is not entitled. I understand the questions on this application and I certify, under penalty of perjury, that the information given by me on this form is correct and complete to the best of my knowledge. I agree to notify this agency of changes in my income, resources, or living arrangements, which might affect my right to receive assistance.
Signature of Applicant or Representative:
Date:
Signature of Applicant’s Spouse or Representative:
Date:
DHR 700 (R. 05/11)
DECLARATION OF CITIZENSHIP/IMMIGRATION STATUS
Georgia Department of Human Services
Division of Family and Children Services
I understand that the Georgia Division of Family and Children Services (DFCS) may require verification from the United States Department of Homeland Security (DHS) of my/my children’s citizenship or immigration status when seeking benefits. Information received from DHS may affect my/my children’s eligibility.
Please fill out and sign ONE or BOTH of the following statements as it pertains to the status of each person seeking benefits.
CHILDREN SEEKING BENEFITS
|
|
U.S. |
Lawfully |
Date Naturalized |
|
|
Citizen |
Admitted |
or Admitted into U.S. |
|
|
|
Immigrant |
|
Name |
Place of Birth(city,state,country) |
(check whichever applies) |
(If applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I, ________________________ attest to the identity of the child/children listed above and
(PRINT NAME)
certify under penalty of perjury, that the information written and checked above is true.
____________________________________ |
________________________ |
||||
SIGNATURE (PARENT/GUARDIAN) |
|
(DATE) |
|
||
|
|
|
|
|
|
|
ADULT(S) SEEKING BENEFITS |
|
|||
|
|
U.S. |
|
Lawfully |
Date Naturalized |
|
|
Citizen |
|
Admitted |
or Admitted into U.S. |
|
|
|
|
Immigrant |
|
Name |
Place of Birth(city,state,country) |
(check whichever applies) |
(If applicable) |
||
|
|
|
|
|
|
|
|
|
|
|
|
I, ________________________ certify under penalty of perjury, that the information
(PRINT NAME)
written and checked above is true. |
|
____________________________________ |
________________________ |
SIGNATURE (PARENT/GUARDIAN) |
(DATE) |
______________________________________________________ |
_____________________________________ |
SIGNATURE (PARENT/GUARDIAN) |
(DATE) |
Form 216 (R. 05/11)
1. Accuracy is essential. Carefully read the entire application and answer each question truthfully. If necessary, attach additional pages for more detailed responses.
2. Submission location matters. Mail or deliver the completed application to your local County Department of Family and Children Services (DFCS) office. Ensure that you include the correct address and attention line.
3. Be prepared for a follow-up. A telephone interview may be required after you submit your application. Provide a reliable phone number where you can be reached.
4. Expect a review process. A DFCS Medicaid Specialist will evaluate your application. If you may qualify for full Medicaid coverage, they will reach out for further information and verification.
5. Personal assistance is allowed. You can have someone help you fill out the application. Ensure that their information is included if they are acting on your behalf.
6. Include all relevant personal details. Provide comprehensive information about yourself and your spouse, including names, birthdates, Social Security numbers, and citizenship status.
7. Disclose all assets and income. List all resources, such as bank accounts, properties, vehicles, and any income you or your spouse receive. This includes Social Security, pensions, and other benefits.
8. Understand your rights and responsibilities. By signing the application, you agree to cooperate with the verification process and report any changes in income or resources that may affect your eligibility.
9. Be aware of estate recovery. Medicaid benefits may be subject to recovery from your estate after your death if you are 55 or older or if you receive certain services. Acknowledge this by signing the appropriate section of the application.
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Georgia Application for Medicaid is used to apply for Medicaid and Medicare Savings programs for qualified beneficiaries, including QMB, SLMB, and QI-1. |
| Submission Instructions | Applicants must read the form carefully, answer all questions accurately, and mail or deliver the application to their local County DFCS office. |
| Interview Requirement | A telephone interview may be required after submitting the application, depending on the applicant's situation. |
| Governing Laws | The application process is governed by federal and state laws, including the Social Security Act and Georgia Medicaid regulations. |